Thoracic Scoliosis with Spinal Instrumentation: Structural Correction, Pulmonary Mechanics, and Long-Term Biomechanical Considerations
Severe thoracic scoliosis is a three-dimensional deformity with direct implications for rib cage geometry, pulmonary mechanics, and global spinal balance. While radiographic correction following spinal instrumentation is often evaluated by Cobb angle reduction, structural alignment alone does not define functional outcome.
A comprehensive evaluation must include respiratory physiology, thoracic mobility, long-term tissue adaptation, and biomechanical durability.
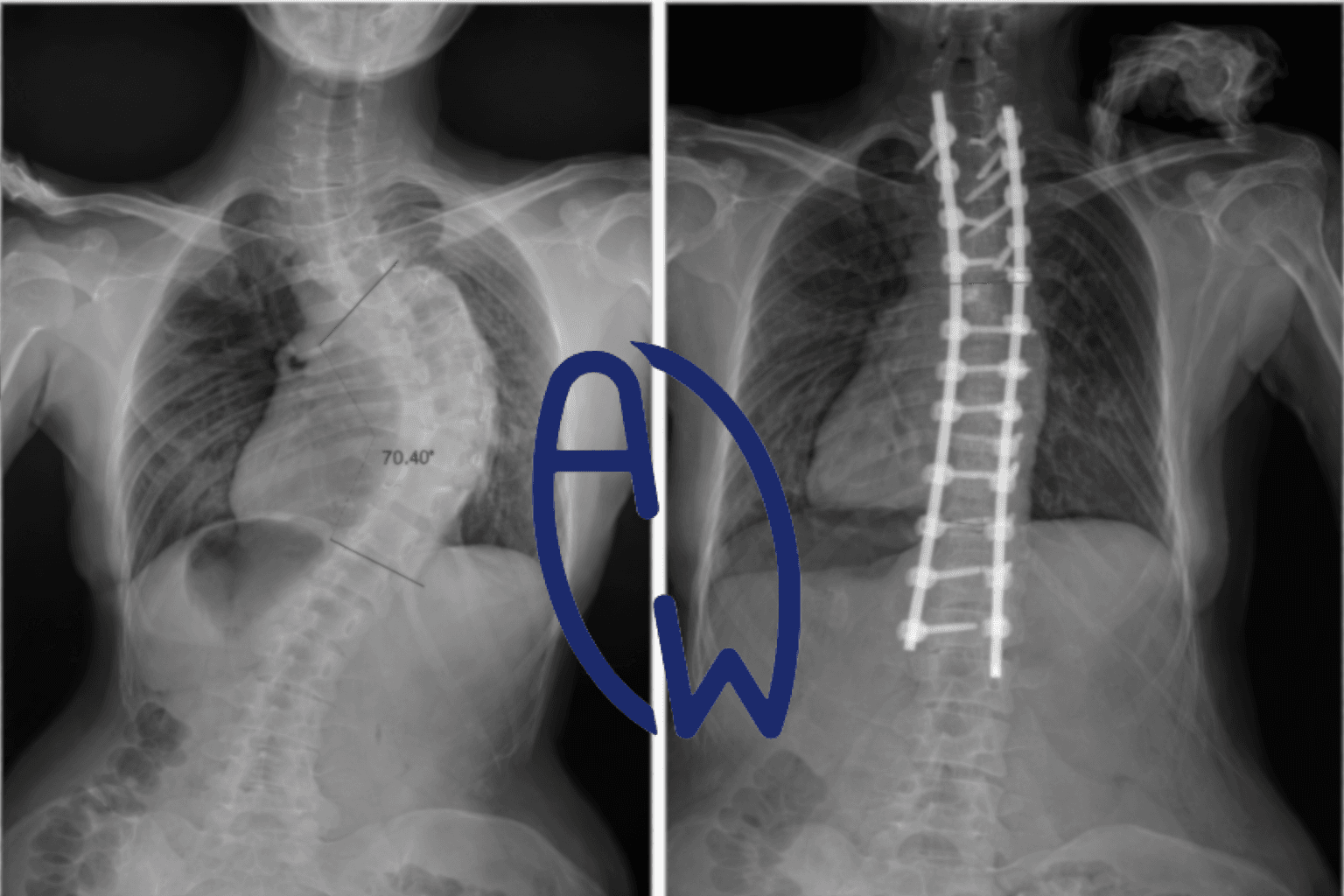
Pre-Operative State: Severe Thoracic Curve (~70–80°)
In severe thoracic scoliosis exceeding 70°, radiographs typically demonstrate:
-
Significant lateral deviation (coronal plane)
-
Vertebral axial rotation
-
Rib prominence on the convex side
-
Rib crowding and chest wall compression on the concave side
As vertebrae rotate, the ribs follow due to costovertebral articulation. This results in asymmetric thoracic cavity dimensions and reduced hemithoracic volume on the concave side.
The deformity is not isolated to bone alignment — it alters the entire thoracopulmonary unit.
Pulmonary Consequences of Thoracic Deformity
Multiple studies have demonstrated that severe thoracic scoliosis produces a restrictive ventilatory defect characterized by reduced:
-
Forced vital capacity (FVC)
-
Total lung capacity (TLC)
-
Chest wall compliance (1,2)
The primary mechanism is mechanical restriction rather than intrinsic pulmonary pathology. The lung parenchyma is generally normal; however, expansion is limited by:
-
Rib cage rigidity
-
Decreased intercostal spacing
-
Altered diaphragmatic mechanics
-
Thoracic rotation
Long-standing deformity may impair ventilation-perfusion matching and increase work of breathing (3).
In adolescents, timing is particularly important. Severe early deformity may influence maximal lung development, as thoracic growth and alveolar multiplication continue through late adolescence (4).
Post-Operative Radiographic Correction
Spinal instrumentation and fusion aim to:
-
Reduce curvature magnitude
-
Correct axial rotation (partially)
-
Prevent progression
-
Restore coronal and sagittal alignment
Post-operatively, Cobb angle reduction is often substantial.
However, thoracic spinal fusion introduces biomechanical consequences:
-
Reduced segmental motion
-
Decreased rib-spine coupling
-
Persistent chest wall stiffness
-
Altered load distribution
Pulmonary function studies show variable outcomes. Some patients experience modest improvement in lung volumes; others demonstrate stabilization rather than normalization (5,6).
Radiographic correction does not guarantee restoration of physiological lung capacity.
Cervical and Global Compensation Patterns
Severe thoracic deformity induces adaptive changes throughout the kinetic chain. Cervical lateral flexion, forward head translation, and shoulder asymmetry are frequently observed compensatory mechanisms.
These adaptations serve critical functions:
-
Maintenance of horizontal gaze
-
Optimization of airway alignment
-
Preservation of balance
Accessory respiratory muscles (sternocleidomastoid, scalenes, upper trapezius) may become chronically overactive when diaphragmatic efficiency is compromised (7).
Thus, cervical symptoms should be interpreted as adaptive responses rather than isolated pathology.
Long-Term Biomechanical Reality: Nothing Is Static
Over time, even spinal rods may demonstrate subtle contour changes. This does not necessarily represent surgical failure. Rather, it reflects biomechanical reality.
The spine remains a living structure:
-
Bone remodels according to Wolff’s Law
-
Adjacent segments adapt
-
Soft tissues respond to load
-
Metal endures cyclical stress
No intervention — surgical or conservative — exists outside the influence of time and mechanical forces.
Long-term studies indicate that adjacent segment degeneration, thoracic stiffness, and altered load transfer may occur following fusion (8).
Similarly, conservative management requires sustained neuromuscular adaptation and compliance to maintain correction.
There is no permanent “fix.”
There is only ongoing adaptation.
Every Treatment Pathway Carries Consequences
Surgical intervention may:
-
Correct magnitude and prevent progression
-
Improve cosmetic alignment
-
Stabilize severe deformity
But it may also:
-
Reduce thoracic mobility
-
Alter respiratory mechanics
-
Shift stress to adjacent segments
Conservative treatment may:
-
Preserve mobility
-
Encourage muscular symmetry
-
Support functional breathing patterns
But it requires:
-
Long-term consistency
-
Active patient participation
-
Ongoing monitoring
The distinction is not between “easy” and “difficult.”
It is between different long-term biomechanical commitments.
Clinical Responsibility: Ask Long-Term Questions
Patients and parents should be encouraged to ask:
-
What are the 10–20 year pulmonary implications?
-
How will thoracic fusion affect aging biomechanics?
-
What is the long-term rehabilitation plan?
-
How is respiratory function being monitored?
-
What functional outcomes are expected beyond radiographic correction?
Informed consent should extend beyond immediate surgical success to lifetime functional sustainability.
Lifelong Functional Consideration
Spinal alignment today must support:
-
Adulthood
-
Pregnancy
-
Occupational loading
-
Aging physiology
Short-term radiographic correction should not overshadow long-term physiological adaptability.
The human body is dynamic.
Correction is structural.
Adaptation is continuous.
Responsibility is lifelong.
Conclusion
Severe thoracic scoliosis is a complex three-dimensional deformity affecting spinal alignment, rib cage geometry, and pulmonary mechanics.
Spinal instrumentation provides essential structural correction in appropriate cases. However:
-
Radiographic improvement does not equate to complete functional normalization.
-
Pulmonary restriction may persist despite alignment correction.
-
Cervical and global compensations reflect adaptive physiology.
-
Long-term biomechanical changes are inevitable.
Optimal patient outcomes require:
-
Structural stabilization when indicated
-
Functional respiratory assessment
-
Post-operative or conservative rehabilitation
-
Lifelong musculoskeletal stewardship
The spine is not a short-term project.
It is a lifetime responsibility.
Your body remains your only permanent home.
References
-
Koumbourlis AC. Scoliosis and the respiratory system. Paediatr Respir Rev. 2006.
-
Weinstein SL, et al. Natural history of adolescent idiopathic scoliosis. J Bone Joint Surg Am. 1981.
-
Newton PO, et al. Pulmonary function in adolescent idiopathic scoliosis. Spine. 2005.
-
Narayanan UG, et al. Thoracic insufficiency and early-onset scoliosis. J Pediatr Orthop. 2014.
-
Kim YJ, et al. Pulmonary function following surgical correction of thoracic scoliosis. Spine. 2007.
-
Johnston CE, et al. Pulmonary function after early thoracic fusion. J Bone Joint Surg Am. 2011.
-
Kapandji IA. The Physiology of the Joints: Volume 3 – The Trunk and the Vertebral Column.
-
Hilibrand AS, et al. Adjacent segment degeneration following spinal fusion. Spine. 1999.
Medical Disclaimer
This article is for educational purposes only and does not constitute medical advice.
Scoliosis varies significantly between individuals. Always consult a qualified healthcare professional before starting any new sport or exercise program, especially if you have scoliosis, spinal conditions, pain, or previous injuries. Participation in sports should be guided by individual assessment and professional recommendation.
The image is shared for educational purposes with patient consent. Individual outcomes vary. Structural correction does not automatically restore full respiratory function. Clinical assessment is required.
Copyright & Content Protection Notice
© 2026 All Well Scoliosis Centre. All rights reserved.
This content is original and protected by copyright law.
No part of this article may be reproduced, distributed, copied, or reused in any form without prior written permission. Unauthorized use, duplication, or content scraping is strictly prohibited.