Mastering Leg Length Discrepancy Analysis: Why a “Short Leg” Is Not Always a Short Bone
Understanding Structural vs Functional Leg Length Difference, Pelvic Mechanics, and Whole-Body Compensation
One of the first lessons we learn in clinical practice is this:
What we see is not always the same as what is actually happening.
A patient may appear to have one leg shorter than the other. The pelvis may look tilted. The shoulders may compensate. The spine may even develop a curve to adapt.
But before concluding someone has a “short leg,” we need to ask an important question:
Is the leg truly shorter — or is the body creating the appearance of a difference?
This is where understanding true leg length discrepancy vs functional leg length discrepancy becomes essential.
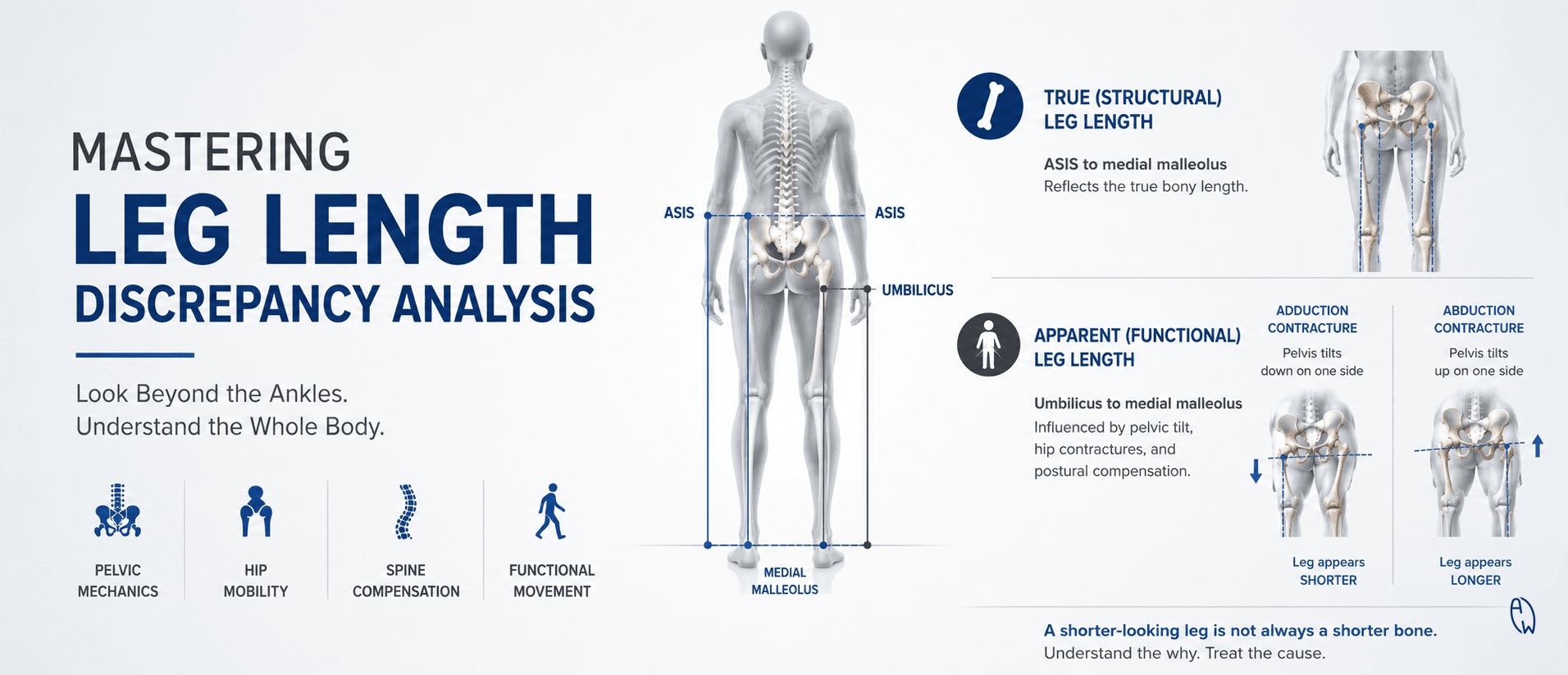
What Is True (Structural) Leg Length Discrepancy?
A true leg length discrepancy refers to an actual anatomical difference in the length of the bones.
This may involve differences in:
-
Femur length (thigh bone)
-
Tibia length (shin bone)
-
Growth-related changes
-
Previous fractures or injuries
-
Joint degeneration or surgery history
Traditionally, clinicians may estimate true leg length by measuring:
Anterior Superior Iliac Spine (ASIS) → Medial Malleolus (inside ankle bone)
This gives an idea of the anatomical distance between the pelvis and ankle.
However, it is important to understand:
A tape measurement is a clinical clue — not a final diagnosis.
Soft tissue tension, difficulty locating landmarks, pelvic rotation, and positioning differences can influence accuracy.
For precise confirmation, especially when treatment decisions depend on millimeters, imaging such as a standing full-length X-ray provides a more objective measurement.
Apparent (Functional) Leg Length Difference: When the Body Creates the Illusion
Sometimes both leg bones are actually the same length — but one leg appears shorter.
This is called a functional or apparent leg length discrepancy.
Instead of a bone-length problem, the difference may come from changes in:
-
Pelvic alignment
-
Hip position
-
Muscle imbalance
-
Joint restrictions
-
Spinal compensation
-
Foot mechanics
A common clinical measurement compares:
Umbilicus → Medial Malleolus
Because this measurement starts from the center of the body, it can reveal how pelvic positioning affects the appearance of leg length.
The Pelvis: The Missing Piece in Leg Length Assessment
The pelvis acts as the bridge between the spine and legs.
Small changes in pelvic position can create significant changes in how the legs appear.
For example:
Hip Adduction Contracture
When the hip is held toward the midline, it can create pelvic compensation and make one side appear shorter — even when the actual bone length is equal.
Hip Abduction Contracture
When the hip is positioned outward, the pelvis may shift differently, creating the appearance of a longer leg.
But hip motion is not only side-to-side.
The body works in three dimensions.
Hip flexion, extension, rotation, spinal posture, muscle tension, and even breathing mechanics can influence how the pelvis organizes itself.
Without looking at the whole picture, we risk treating the measurement instead of understanding the person.
Why Standing Assessment Matters
The human body functions under gravity.
A person does not walk, run, or live lying on an examination table.
This is why assessing leg length only in a non-weight-bearing position can miss important information.
A commonly used clinical assessment is the:
Standing Block Test
Small blocks are placed under the apparently shorter side until pelvic balance improves.
During this process, clinicians observe:
-
Pelvic leveling
-
Walking pattern
-
Spinal compensation
-
Hip mobility
-
Knee alignment
-
Foot posture
-
Muscle adaptation
This helps answer a more practical question:
How much difference is the body actually experiencing during daily movement?
Leg Length Difference and the Spine
The spine is highly adaptable.
When the pelvis is uneven, the spine may compensate by creating changes such as:
-
Lumbar side bending
-
Postural imbalance
-
Uneven loading patterns
-
Muscle asymmetry
However, not every pelvic tilt means someone needs a heel lift.
The key is determining whether the imbalance is:
Structural → caused by actual bone length difference
or
Functional → caused by how the body is adapting
The treatment approach is completely different.
Measure Twice. Understand First.
Leg length assessment is not about simply looking at the ankles and deciding one leg is shorter.
The medial malleoli may tell part of the story — but not the whole story.
A complete evaluation considers:
✓ Bone structure
✓ Pelvic mechanics
✓ Hip mobility
✓ Spine compensation
✓ Muscle function
✓ Standing posture
✓ Movement patterns
✓ Imaging when clinically necessary
Because the goal is not just to “make the legs equal.”
The goal is to understand why the body adapted in the first place.
A short leg is sometimes a bone problem.
Sometimes it is a pelvic story.
Sometimes it is a whole-body adaptation.
The best assessment begins by understanding the difference.